

Traumatic C2 Spondylolisthesis
Traumatic C2 spondylolisthesis (hangman fracture) results from a combination of axial loading and either hyperextension or hyperflexion. It is usually seen in high-speed motor vehicle accidents. Both C2 pedicles fracture with varying degrees of angulation and anterolisthesis of C2 on C3. Neurologic sequelae are uncommon. Because the fracture tends to widen, rather than narrow, the spinal canal, the spinal cord and nerve roots are not usually damaged. The “atypical” hangman fracture is a variant in which the coronal fracture traverses the posterior C2 body, rather than the pedicles. The most common classification scheme is that of Levine and Edwards after Effendi.
Effendi/Levine Edwards classification
Type I
Bilateral pedicle fractures with intact disk and ligaments. No angulation or translation
Type II
C2/3 disk disruption with angulation but no translation
Type III
C2/3 disk disruption with angulation, translation, and facet subluxation or dislocation
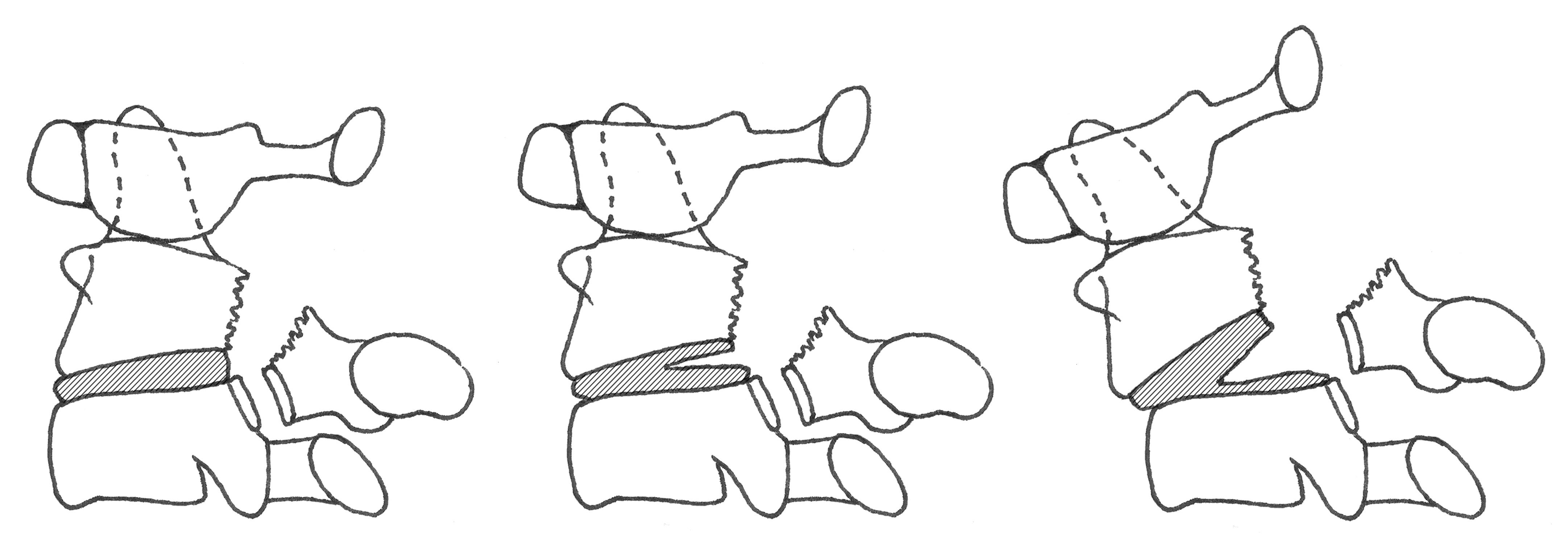
Type I fractures are stable, types II and III are unstable
CT permits accurate evaluation of displacement and angulation, which impact classification and treatment decisions. MRI optimally evaluates disc and ligamentous integrity. Vertebral foraminal fractures indicate potential vascular injury and head/neck CTA should be considered to exclude occult vertebral or carotid artery injury.
Fractures that do not show disk widening, angulation, or subluxation (Type 1) are considered stable.

Type I hangman fracture. Nondisplaced pedicle fractures with normal C2–C3 alignment and no disk space widening, translation, or angulation.




Type III hangman fracture. Anterior angulation and widening of C2–C3 disk space. Bilateral pedicle fractures with C2–C3 facet subluxation. T2-weighted sagittal MRI shows C2–C3 disk disruption and extensive prevertebral and nuchal ligament edema.