

Tracheobronchial rupture is rarely encountered in clinical practice because most patients with this injury die from respiratory failure or exsanguination before arriving at the emergency department. In blunt trauma, abrupt deceleration and intrathoracic shearing forces as well as compression of the airways between the sternum and thoracic spine can disrupt the trachea or mainstem bronchus. Most injuries occur within 2.5 cm of the carina.
The most common imaging findings are pneumomediastinum and pneumothorax. Persistent pneumothorax after chest tube placement and suction is the hallmark of a major bronchial injury. With complete bronchial transection, the ipsilateral lung falls to the dependent (usually posterior) portion of the hemithorax; the “fallen lung” sign.

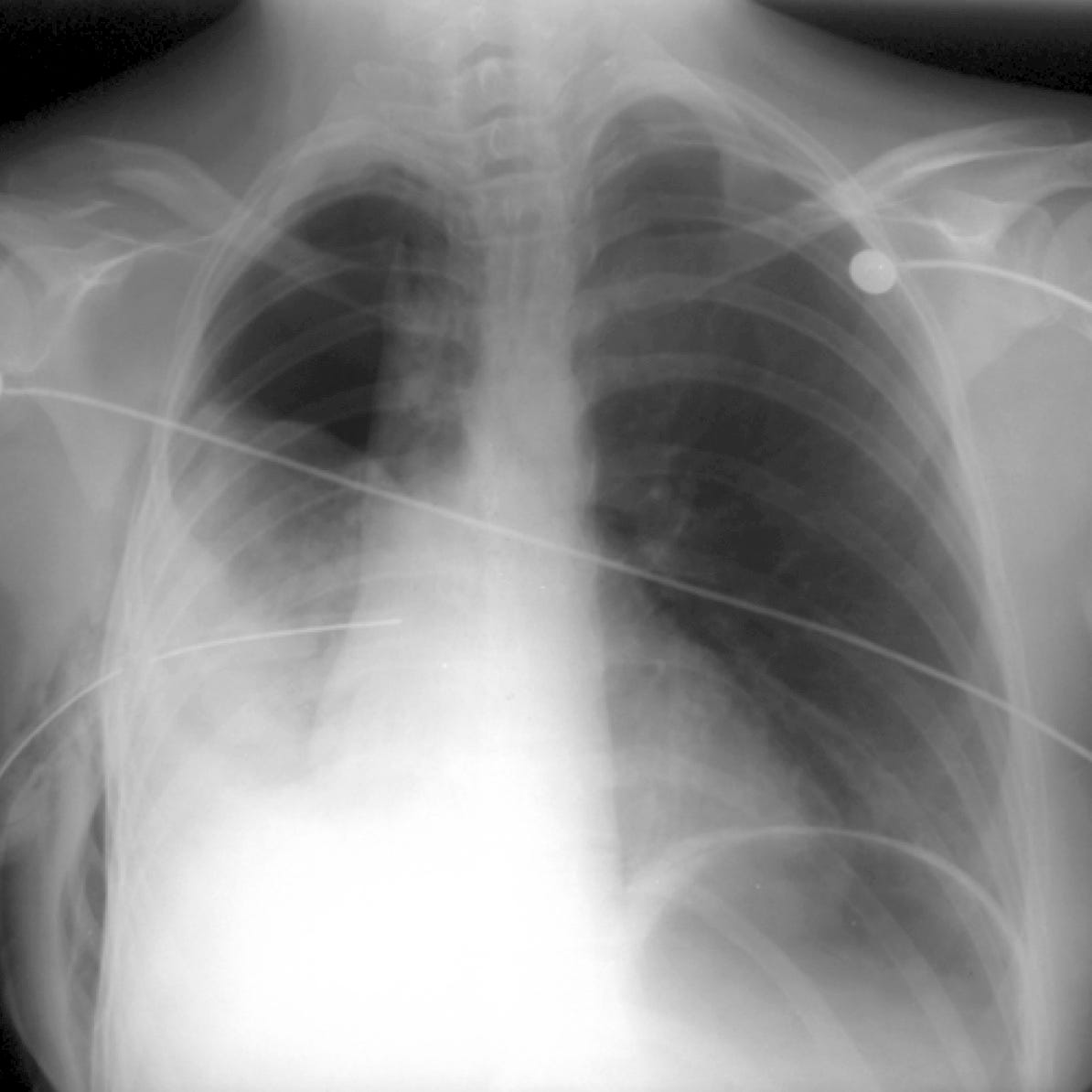
Bronchial rupture. The right lung is collapsed about the hilum and inferiorly positioned in the chest. Large right pneumothorax
Bronchial rupture. Persistent large pneumothorax following chest tube placement.
Chest CT can identify the exact site of the tear as a focal or a circumferential defect in the tracheal or bronchial wall. Other imaging findings include airway contour deformity, extraluminal endotracheal tube tip position, herniation or overdistension of the balloon, pneumomediastinum, and deep cervical soft tissue emphysema.