
Pyloric stenosis
Pediatrics

Pyloric stenosis is idiopathic hypertrophy of the pylorus muscle, leading to gastric outlet obstruction. It is more common in males than in females and usually presents between 3 and 6 weeks of age with gradual onset of non-bilious projectile vomiting. Occasionally the hypertrophied pylorus muscle can be palpated as an olive-sized mass in the upper right quadrant.
Abdominal radiographs in pyloric stenosis may show a dilated, gas-filled stomach. Ultrasound is diagnostic; the pyloric channel is thickened and elongated with a length exceeding 12 mm and muscle thickness greater than 3 mm.
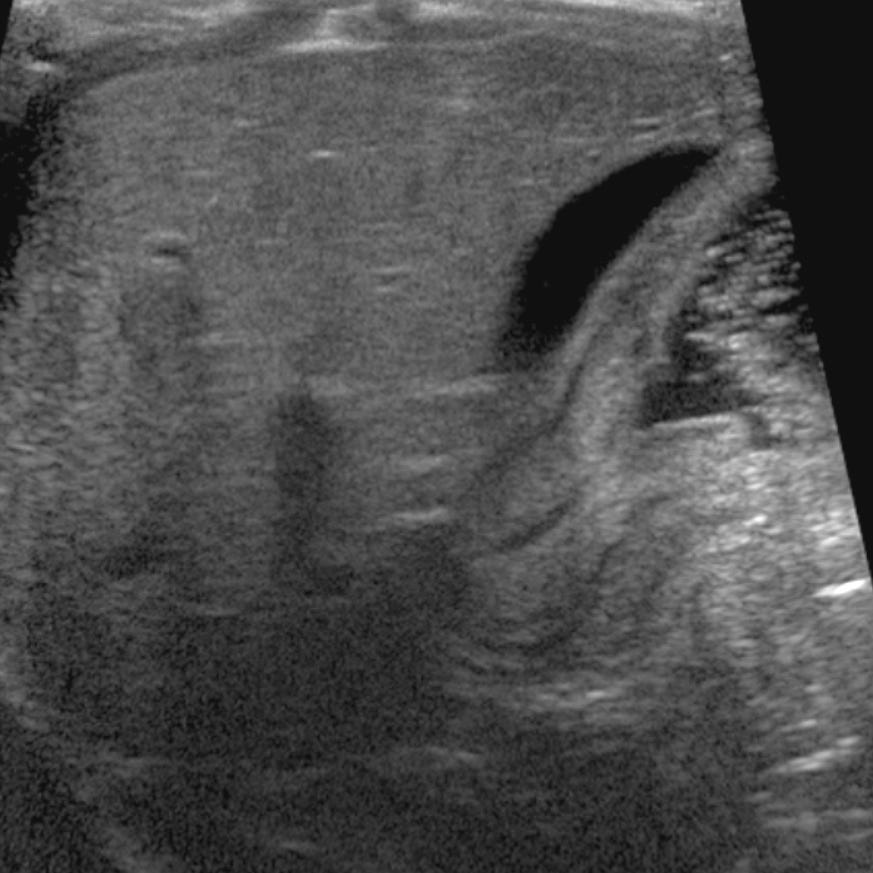
Pyloric stenosis. The pylorus is thickened and elongated measuring 18 mm in length and 6 mm in wall thickness. The hypoechoic structure superior to the pylorus/gastric antrum is the gallbladder. The stomach is to the upper left of the pylorus and contains echogenic material.
Emergent management consists of bowel rest, volume resuscitation, and correction of any electrolyte abnormalities. Definitive treatment is surgical pyloromyotomy
.
Yes. Simple fluid, like bile in the gallbladder, or fluid in a cyst does not have anything to reflect ultrasound waves back to the detector, so it appears black, with brighter reflection in the tissues beyond it, further from the transducer.
Hypoechoic things are black?