

Pulmonary contusion
Pulmonary contusions are usually a consequence of blunt chest trauma and reflect a combination of focal parenchymal injury, edema, and interstitial and alveolar hemorrhage. Radiographic findings range from irregular nodular opacities to large areas of consolidation, but plain films are often nonspecific; aspiration pneumonitis can have a similar appearance and can also be seen in trauma. On CT, pulmonary contusions appear as focal peripheral lung opacity adjacent to an area of impact. Posterior and lower lobes are more commonly affected.
In contrast to lobar pneumonia, pulmonary contusions do not respect fissures and do not localize to a segment. They may be widespread, and simulate ARDS or alveolar edema. In most cases, pulmonary contusion is apparent on the initial examination and does not worsen in severity. Pulmonary contusions clear rapidly on radiographs and can resolve in as few as 72 hours.


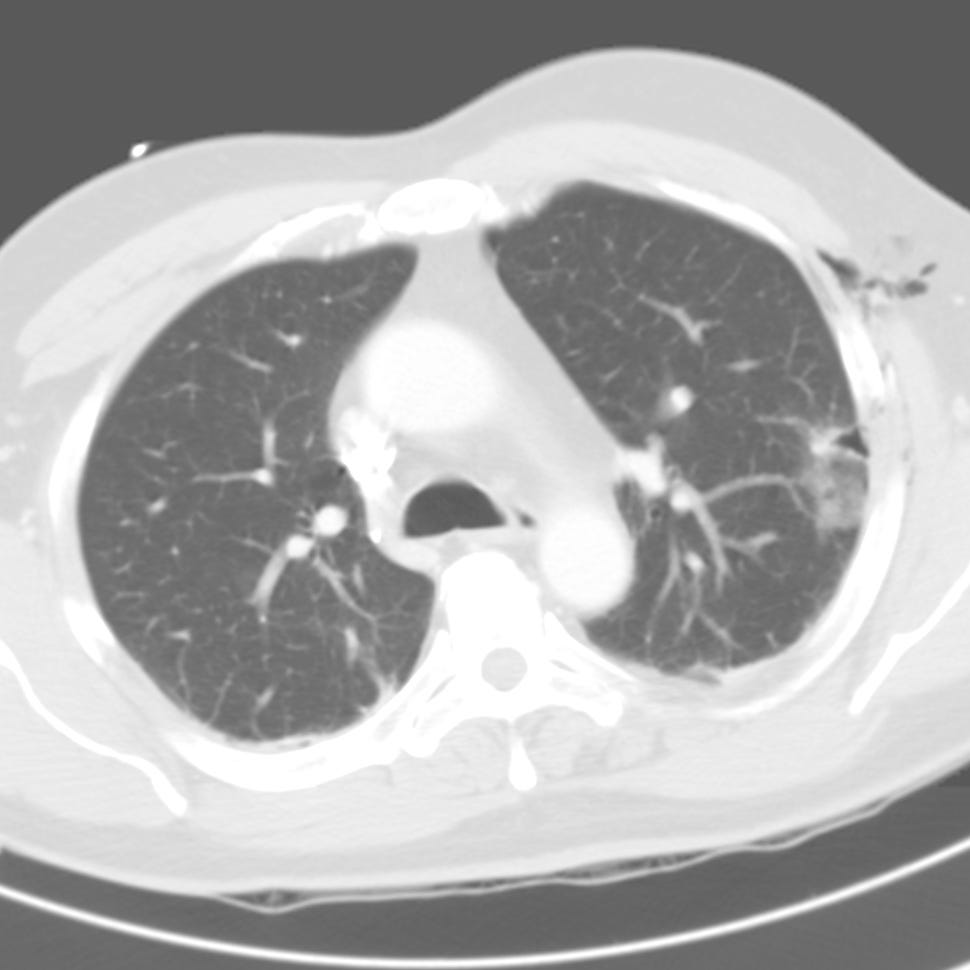
Pulmonary contusion. Focal anterior segment left upper lobe and right perihilar airspace opacification (contusion). Small right pneumothorax. Right thoracostomy tube located in the major fissure. Right axillary soft tissue emphysema.

Lingular contusion. Left hemothorax and subcutaneous emphysema

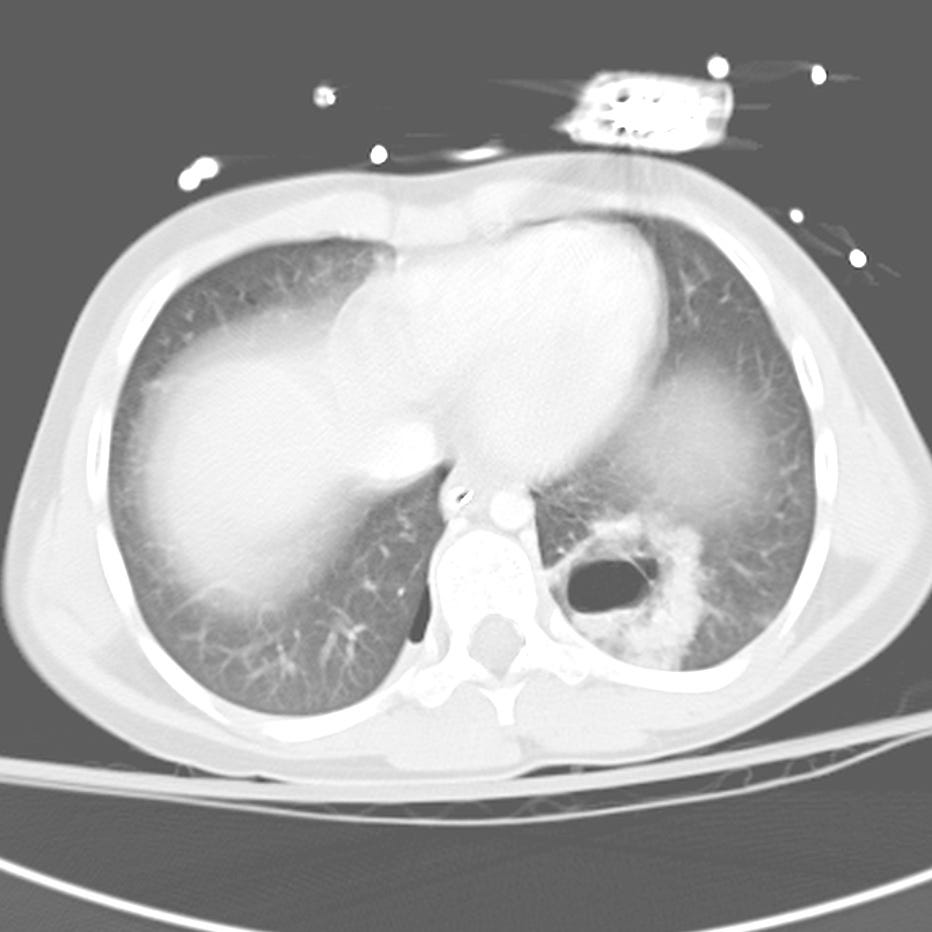
Bilateral lower lobe contusions. Right hemothorax. Subcutaneous emphysema.
Pulmonary Laceration
Pulmonary lacerations reflect traumatic disruption of the lung parenchyma with hematoma or pneumatocele formation. They are the consquence of shearing forces and are seen in blunt and penetrating injury, and are often obscured by adjacent pulmonary contusion, hemothorax, or pneumothorax. Pulmonary lacerations are easily missed on portable chest radiographs; most acute lacerations are detected with CT and appear as discrete round or oval air or fluid collections surrounded by consolidation.
There are four types of pulmonary laceration:
Type 1 (compression rupture injury) is most common and due to sudden compression of the chest wall with rupture of the inflated lung parenchyma.
Type 2 (compression shear injury) results from compression of the lower chest with displacement of the lower lobe across the spine, causing a juxtavertebral cavity.
Compression shear pulmonary laceration (Type 2). Left lower lobe round paravertebral air collection within a larger area of air space opacity. Small right posterior hemopneumothorax.
Type 3 (rib penetration tear) is a small peripheral laceration adjacent to a rib fracture.
Rib penetration tear pulmonary laceration (Type 3). Small peripheral pneumatocele adjacent to left rib fracture.
Type 4 (adhesion tear) occurs at the location of a preexisting pleuropulmonary scar .