

Laryngeal fractures are rare, and most are due to blunt trauma from motor vehicle and sports injuries, although penetrating injuries do occur. The larynx is necessary for maintaining airway patency and protection, swallowing, and phonation; consequences of laryngeal fracture or injury include airway obstruction, aspiration, and vocal dysfunction. Complete laryngo-tracheal separation is generally fatal unless immediately detected and stabilized. The primary goal of emergency management is to protect the airway, which may require intubation or tracheostomy.
Clinical findings in laryngeal trauma include subcutaneous emphysema and loss of the normal tracheal prominence. Careful attention to the laryngeal skeleton on CT examination, particularly in intubated patients, detects laryngeal fractures, which can be managed by early tracheostomy and surgical repair. In polytrauma patients, hyoid, cricoid, and thyroid cartilage fractures can be easily overlooked and diagnosis delayed for days or weeks, until the patient is extubated and late complications such as dysphonia or aspiration become apparent.
Patients who can cooperate with clinical examination may present with dyspnea, dysphonia, hoarseness, dysphagia, odynophagia, neck pain, or hemoptysis. These symptoms should prompt laryngoscopy and CT imaging.
CT findings include cartilage discontinuity, soft tissue asymmetry, subcutaneous and deep space emphysema, submucosal edema, and laryngeal hematoma.


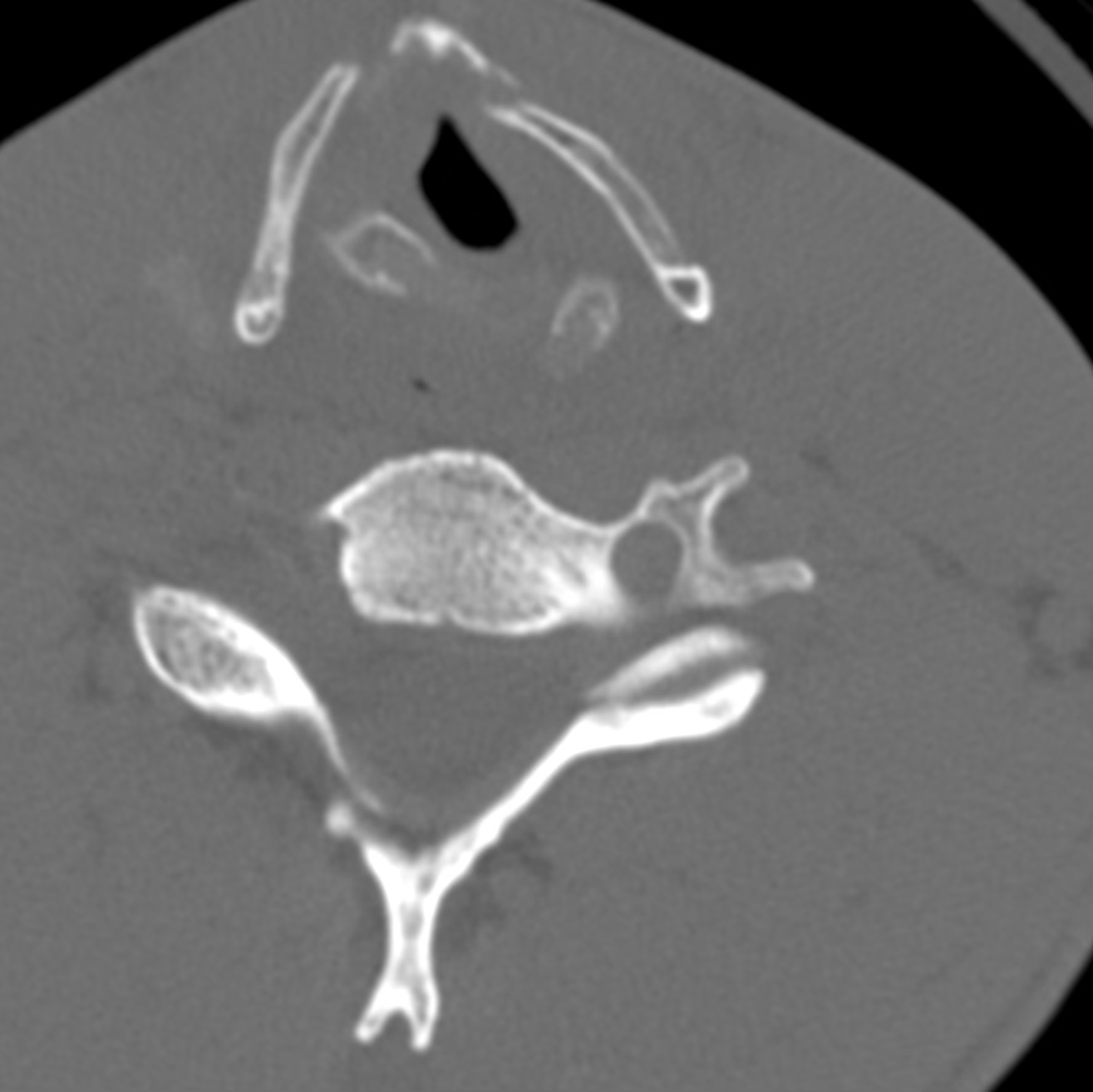
Hyoid and thyroid cartilage fractures. Right hyoid and thyroid cornua fractures. Moderate laryngeal edema
Thyroid and cricoid cartilage fractures. Bilateral anterior thyroid cartilage fractures, with grossly displaced cricoid fracture and associated soft tissue edema.
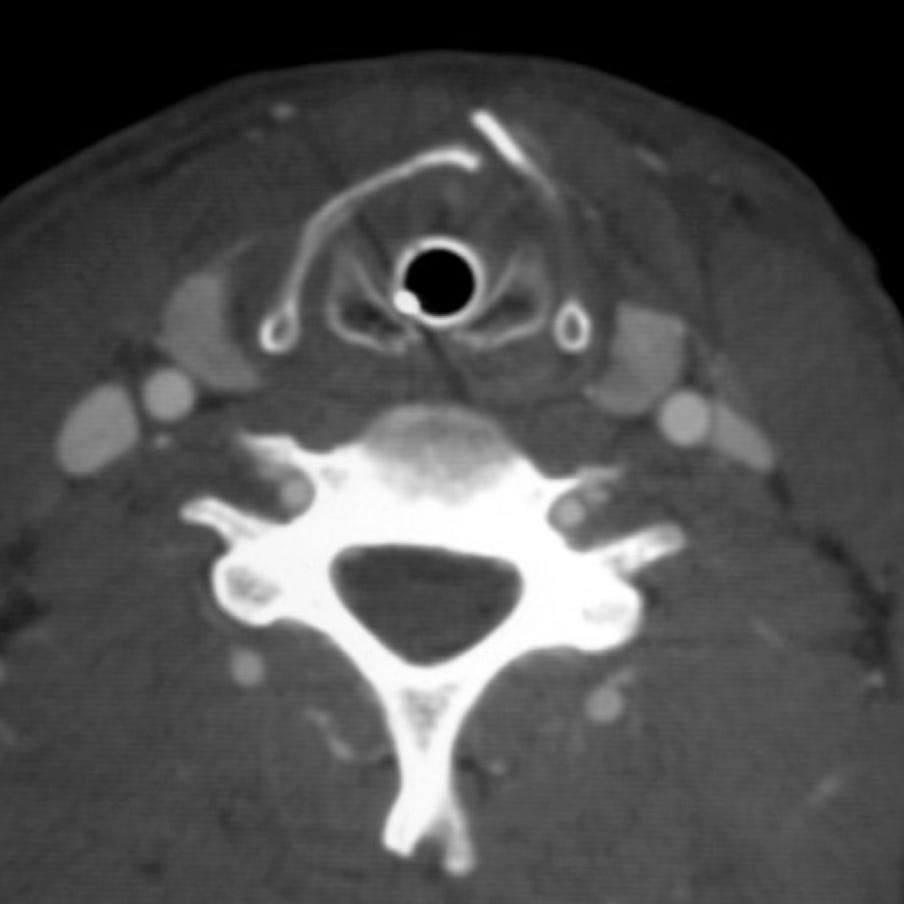
Thyroid and cricoid cartilage fractures in an intubated patient. Anterior thyroid cartilage and posterior cricoid fractures.