



Duodenal atresia, stenosis, or web are the most common causes of proximal bowel obstruction in the neonate. Clinical findings are abdominal distention, vomiting, and failure to pass meconium. In cases of complete atresia, the distal bowel will not contain gas. Because obstruction is usually distal to the pancreatic ampulla, vomiting in duodenal atresia is usually bilious. Associated congenital disorders are common and include Down syndrome and the VACTERL association (vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities).
Radiographs show a dilated stomach and small bowel proximal to the obstruction. The “double bubble” sign corresponds to isolated air-filled distended stomach and duodenal bulb separated by the normal pylorus. Prenatal ultrasonography may also reveal similar findings, but duodenal atresia is often not detectable until the mid to late second trimester. Incomplete duodenal obstruction may show gas in distal bowel loops and is seen with duodenal webs and stenosis. Annular pancreas or volvulus can present with a similar clinical and imaging picture.
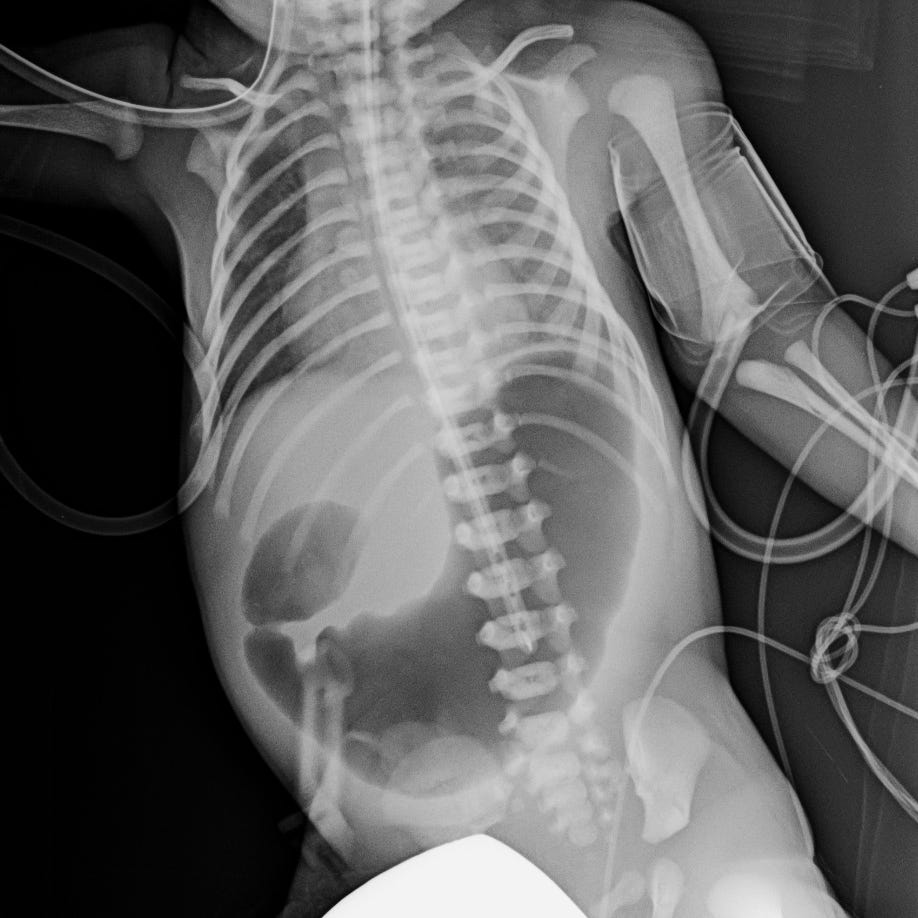
Double bubble sign in complete duodenal atresia. Markedly distended air-filled stomach and proximal duodenum. The remainder of the abdomen is entirely gasless.
Surgical correction is required, and the prognosis is excellent, especially in non- syndromic cases.