

Cerebral contusions result from acceleration injuries in which the brain strikes the irregular surfaces of the orbital roofs, petrous ridges, and sphenoid wings. Most are located in the cortex and immediate subcortical white matter of the inferior frontal lobes, anterior or inferior temporal lobes, posterior cerebellum, dorsal occipital lobes, and frontal and parietal convexities. They may be either coup or contrecoup in location, although the latter are more common. Isolated contusions typically carry a better prognosis than traumatic axonal injury unless associated with significant brain swelling, parenchymal hematoma or extra-axial hemorrhage.
CT is the first and often only investigation in the emergency setting; MRI is more sensitive for detection of small hemorrhages, which can be important for prognosis. Contusions may be subtle or imperceptible immediately following an acute injury, and are not necessarily hemorrhagic. Delayed hemorrhage can occur, usually 12 to 48 hours post-injury, and presents clinically as neurological deterioration sometimes called posttraumatic apoplexy. Late hemorrhage reflects hypocoagulability that often develops following head trauma as well as resolution of acute cerebral swelling that serves to tamponade small vascular injuries. Resolving contusions may show peripheral enhancement on post-contrast CT and MRI, and may mimic tumors, absceses, or subacute infarcts

Hemorrhagic right temporal contusion. Right temporal hematoma with adjacent traumatic subarachnoid hemorrhage. Blood within the left sphenoid sinus indicates associated central skull base fracture.

Nonhemorrhagic right and hemorrhagic left contusions. Low-attenuation edema within the right temporal lobe and hematoma surrounded by vasogenic edema in the left temporal lobe. Generalized brain swelling with cisternal effacement and subtle traumatic subarachnoid hemorrhage in the interpeduncular and quadrigeminal plate cisterns.

Bilateral contusions. Bilateral temporal hemorrhagic contusions and left inferior frontal nonhemorrhagic contusions.
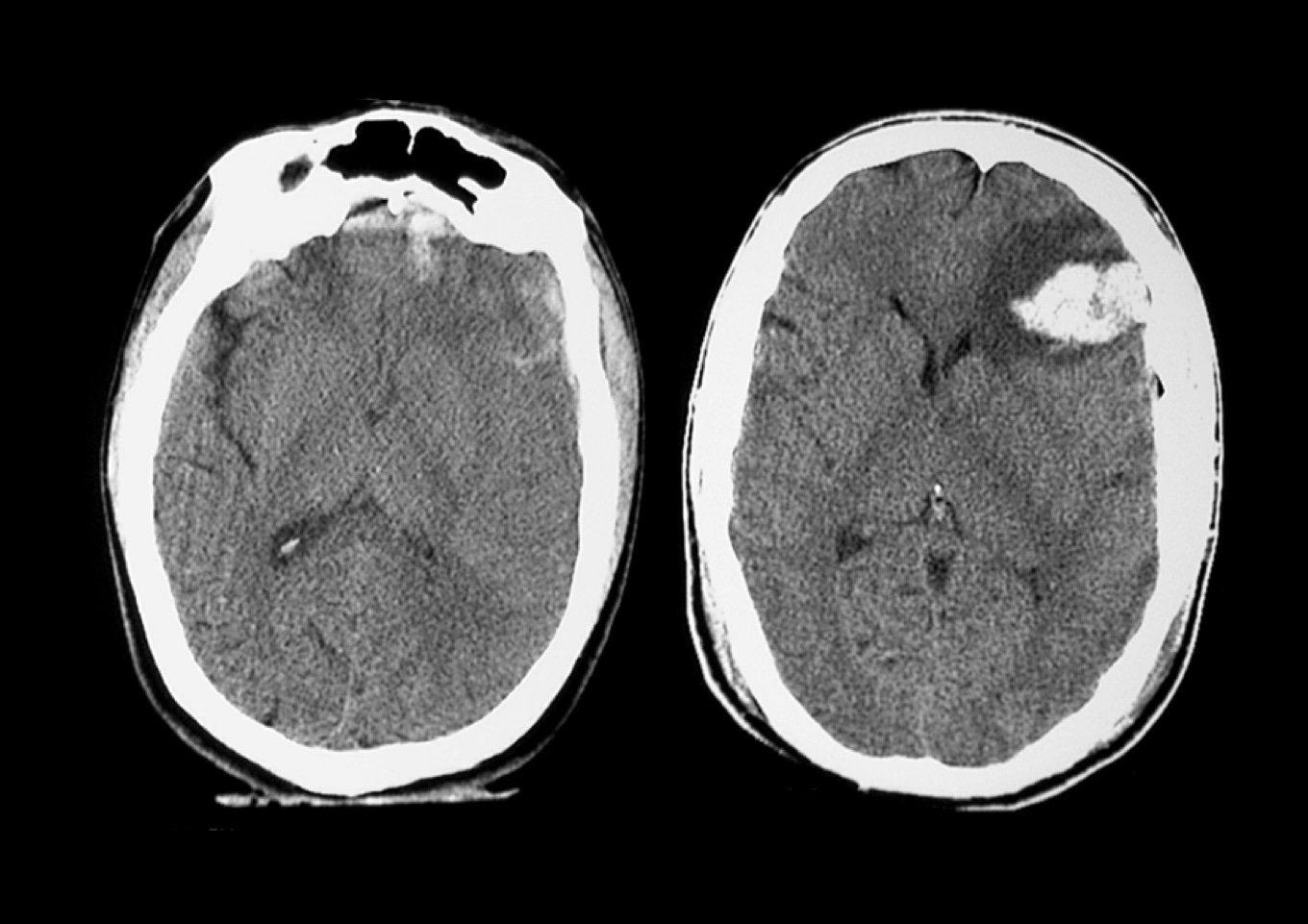
Delayed hemorrhage. Subtle left frontal traumatic subarachnoid hemorrhage and focal edema on the initial (left) image. Subsequent cortical/subcortical hematoma after 24 hours
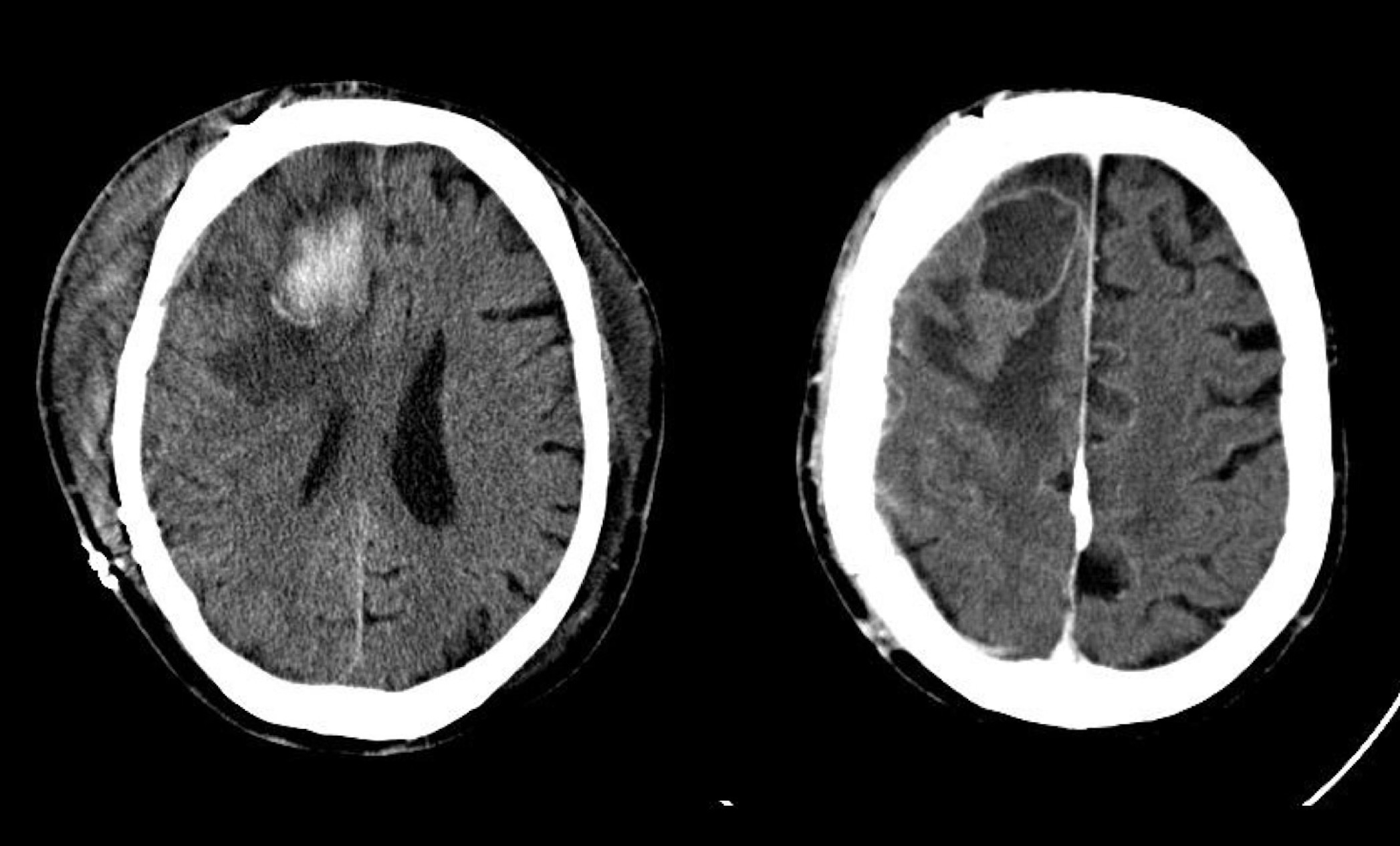
Evolution of cortical contusion/hematoma. Initial examinationb(left)shows extensive scalp swelling and subacute hemorrhagic frontal contusion. Later image demonstrates low attenuation mass with thin peripheral enhancement and surrounding vasogenic edema which could mimic neoplasm or abscess.