

Children, usually between age 1 and 3 years, may ingest or aspirate foreign bodies. Choking, gagging, coughing, unilateral wheezing, and respiratory distress are clinical signs. Large objects can lodge in the larynx or trachea and cause complete airway obstruction with consequent asphyxia or anoxia. Smaller objects will pass beyond the carina with mild or absent acute manifestations, but can cause chronic infection or bronchiectasis if the aspirated material cannot be cleared.
Unless an aspirated foreign body is metallic, it is unlikely to be identified on a chest radiograph. Air trapping, unilateral hyperinflation, lobar or segmental atelectasis, mediastinal shift, or pneumomediastinum are indirect signs of aspiration with bronchial obstruction. In adults, an aspirated object usually passes into the right main bronchus, since it is more vertically oriented with respect to the carina and trachea, however in children, the bronchi are more symmetric, and either can be involved. Unilateral hyperinflation that persists on decubitus positioning (with the hyperinflated side downward) is one sign. Postobstructive atelectasis and pneumonia may also be seen.


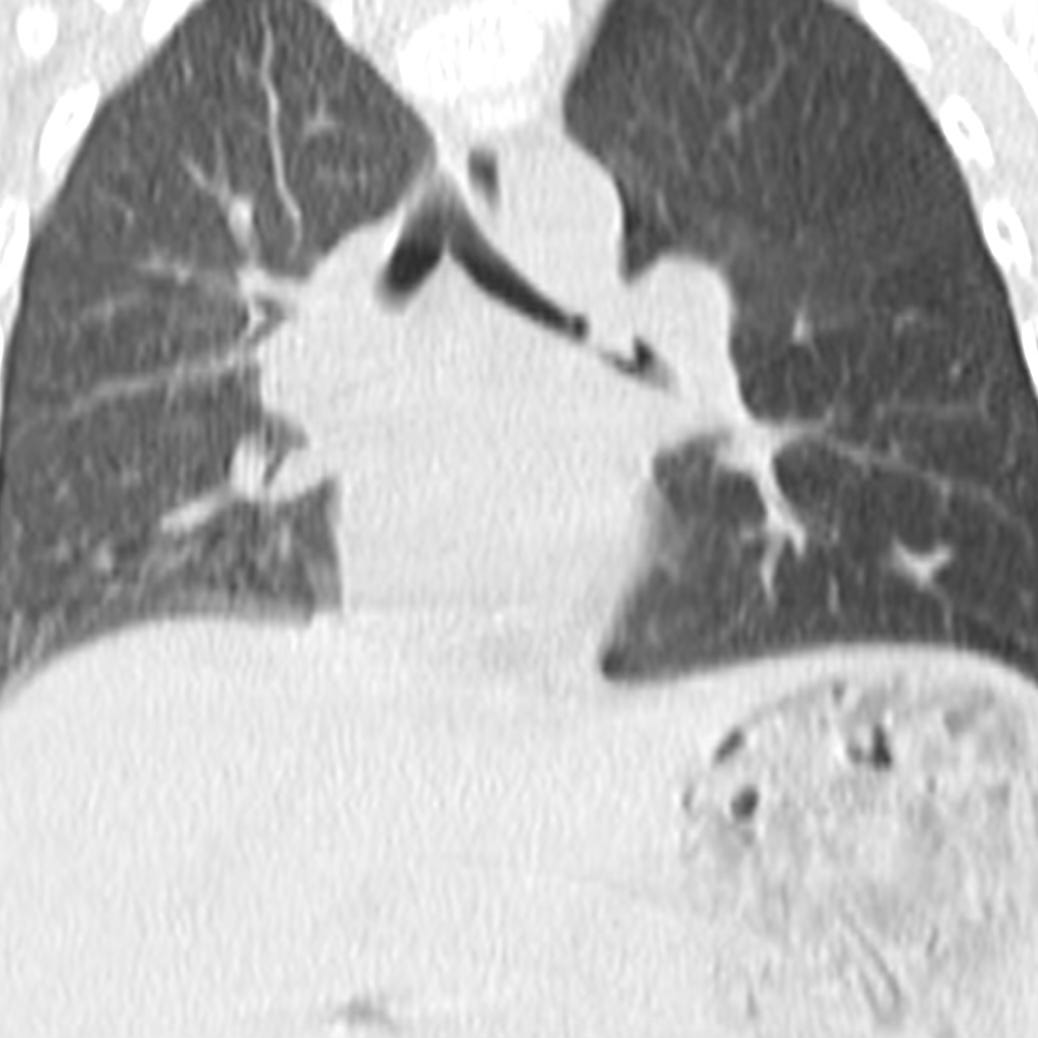
Aspirated turkey burger. Rightward mediastinal shift that persists on left-side-down decubitus radiograph. CT shows foreign body in left mainstem bronchus.
Primary management in the emergency department aims to relieve any airway compromise, and bronchoscopy or endoscopy can effectively retrieve an impacted foreign body. Antibiotics are not indicated except in the case of secondary pulmonary infection.
Many ingested foreign bodies that reach the stomach will eventually pass through the gastrointestinal tract. Perforation and obstruction are risks, particularly with foreign bodies in the esophagus, with sharp objects, and in patients with developmental gastrointestinal anomalies or prior surgery. Emergent endoscopy is indicated for sharp objects or disk batteries lodged in the esophagus and in any patient who cannot manage secretions due to complete esophageal obstruction. Sharp pointed objects, objects greater than 6 cm in length or 2.5 cm in diameter, and magnets in the stomach or duodenum should be removed promptly. In asymptomatic patients, coins in the esophagus can be observed for 48 hours. Disk or cylindrical batteries should be removed if they do not pass from the stomach within 48 hours.


Swallowed coin. A round metallic object is located in the mid-esophagus.